A Five-Year Review of Refractive Procedures, Outcomes and Complications
Robert Edward T. Ang, MD, Clarissa Marie S. Tady, MD, Niccolo Zandro R. Valencia, MD, Lilette Marie B. Canilao, MD, Dennis C. Vizconde, MD, Mark Christian R. Rivera, MD
Refractive surgery encompasses surgical procedures that aim to correct refractive errors and improve vision with less dependence on eyeglasses or contact lens. These include laser-in-situ keratomileusis (LASIK), photorefractive keratectomy (PRK), phakic intraocular lenses (IOLs), and refractive correction for presbyopia.
LASIK is among the most common ophthalmic procedures in the world and its popularity lies in the procedure’s safety, efficacy, quick visual recovery, on top of minimal patient discomfort.1 The surgeon uses either a microkeratome or a femtosecond laser to cut a flap of corneal tissue. The flap is then lifted and a pre-computed amount of tissue is removed from the corneal stroma with an excimer laser after which the flap is subsequently folded back into the cornea. Research conducted by the Magill Research Center for Vision Correction, Medical University of South Carolina, showed that the overall patient satisfaction rate after primary LASIK surgery was 95.4%.2 Another study by Alio evaluated the long-term outcomes of LASIK for high myopia and concluded that it was safe.3
PRK, on the other hand, involves scraping of the corneal epithelium and ablation of corneal tissue to alter the refractive power. Unlike LASIK, PRK does not create a thick corneal flap. This translates to an advantage for PRK over LASIK, where a thicker, intact, structurally stronger cornea is preserved. De-epithelialization is needed for the excimer laser to access stromal tissue and this results in disadvantages, such as postoperative discomfort, delayed visual recovery, and the risk of stromal scarring. Its efficacy in terms of visual outcomes is comparable to LASIK (0.90 for PRK; 0.95 for LASIK).4 A study by Shalchi showed that, although predictability of results may vary, PRK was still safe with no long-term complications.5
In recent years, phakic intraocular lens (IOLs) has been developed as a viable option in refractive surgery. Phakic IOLs are lenses that are inserted either in the anterior or posterior chamber of the eye to correct refractive errors and astigmatism. The advantages of phakic IOLs are the following: (1) it maintains the structural integrity of the cornea, (2) it corrects refractive errors even beyond the range of LASIK, and (3) it does not remove the natural lens and, therefore, has less risk of retinal detachment and macular edema. Phakic IOLs are considered alternatives if corneal refractive procedures are not feasible, such as in patients with inadequate corneal thickness exceeding the safety limits of LASIK, as well as in patients with corneal topographic irregularities. It can even be offered to patients who are qualified for LASIK and PRK but do not want the associated risks involved. The procedure is reversible because the lens can be easily removed if the patient so desires. We use the Visian Implantable Collamer lens (ICL, Staar, USA), which is a posterior chamber phakic intraocular lens inserted into the sulcus over the natural lens. A Cochrane review presented a meta-analysis of three clinical trials that compared keratorefractive surgeries (LASIK, PRK) and phakic IOL implantation for patients with myopia and showed that the percentage of eyes with uncorrected visual acuity (UCVA) of 20/20 was not significantly different between the groups.6
Also gaining popularity, especially in the middle-aged group, are the presbyopic treatment procedures. Among them is the LASIK-based Supracor (Bausch & Lomb, USA), which treats refractive error and presbyopia simultaneously to improve both near and distance vision. It creates an ablation profile wherein there is a 12-micron elevation in the central 3 mm of the cornea surrounded by an aspheric optimized midperiphery to provide a smooth transition from distance to near correction.7 Unlike LASIK, PRK or phakic IOLs where the target refraction is plano (0.00D) to achieve distance vision of 20/20, the recommended target refraction for Supracor is -0.50D which gives an uncorrected near vision of J1 and uncorrected distance vision of 20/30. A study by Saib concluded that Supracor can improve functional near, intermediate, and distance vision in presbyopic patients with low and moderate hyperopia.8
This study reviewed the visual and refractive outcomes of eyes that underwent refractive surgery in a refractive center from 2010 to 2014 and reported the occurrence of complications and the outcomes of remedial measures performed.
Given that refractive surgery is mostly performed on young and healthy eyes of patients with high expectations, it is critical that surgical outcomes are periodically evaluated to determine the long-term safety and efficacy of the procedures. This will allow for continuous adjustment in the nomograms. It can help refractive surgeons anticipate unwanted complications and hopefully prevent them from future occurrences.
METHODOLOGY
This study was approved by the Ethical Committee of Clinical Investigation of Asian Eye Institute and followed the tenets of the Declaration of Helsinki.
Study population
This is a retrospective single-center, single- surgeon study that reviewed the surgical outcomes of refractive procedures performed from January 2010 to December 2014. Inclusion criteria were patients age 18 and above who underwent a full refractive screening, consented and underwent refractive surgery procedures. The data from 1,366 eyes of 771 patients who were treated with LASIK, PRK, phakic IOL, and Supracor with at least 1 month follow up after their surgery were analyzed. Only hyperopic patients who underwent Supracor were analyzed because the myopic algorithm was not commercially available. Exclusion criteria were the presence of previously diagnosed disease of the ocular surface (e.g. keratoconus, ectasia), optic nerve or retina problem that could affect the visual outcome, previous ocular surgery, incomplete screening data, and less than one month postoperative follow up.
Refractive screening
Complete ophthalmologic examinations for refractive screening were performed on all eyes. These included uncorrected and best-corrected visual acuity, manifest refraction, Goldmann applanation tonometry, Schirmer’s test, corneal topography, slit lamp biomicroscopy, and indirect ophthalmoscopy.
Postoperative evaluation
All patients were advised to return for postoperative evaluation at 1 day, 1 week, 1, 3, and 6 months, 1 and 2 years after the initial surgery. Postoperative parameters included uncorrected and corrected distance, intermediate, and near visual acuity (for Supracor), manifest refraction, intraocular pressure, and slit lamp examination of the cornea. Complications that occurred within the five-year time point and their remedial procedures were analyzed.
Enhancement of LASIK, Supracor, and PRK were analyzed independently. Mean time of enhancement, pre-enhancement, and 1 month post-enhancement manifest-refraction spherical equivalent (MRSE) of LASIK, PRK, and Supracor were also collected and analyzed.
Statistical analysis
Descriptive statistics were used to summarize the clinical characteristics of the patients. Frequency and proportion were used for nominal variables, median and IQR for ordinal variables, and mean and SD for interval/ratio variables. Analysis of variance was used to determine the significant difference in three or more groups with interval/ratio variables. Independent t-test was used to determine the statistical difference for uncorrected distance visual acuity (UDVA), best corrected visual acuity (BCVA), and MRSE between LASIK and PRK groups, as well as between femtosecond laser and blade LASIK groups. Null hypothesis was rejected at 0.05 α-level of significance. STATA 12.0 was used for data analysis.
RESULTS
Demographics
This study evaluated 1,366 eyes of 771 patients who underwent various refractive procedures. 59.5% of the participants were females. LASIK, PRK, and phakic IOL belonged to similar age groups with mean ages of 32.31, 31.35, and 27.33 years, respectively, while the Supracor group was older with mean age of 51.05 years (Table1).
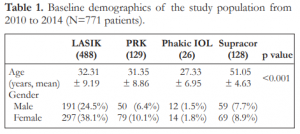
Table 1. Baseline demographics of the study population from 2010 to 2014 (N=771 patients).
Annual breakdown of refractive surgeries
Nine hundred twenty six (926) eyes underwent LASIK (femto and blade), 249 eyes underwent PRK, 51 eyes were implanted with phakic IOLs, and 140 eyes underwent Supracor. LASIK (femto and blade) was the most commonly performed procedure at 68%, followed by PRK (18.3%), Supracor (10.2%), and phakic IOL (3.7%). In 2010, more eyes underwent blade LASIK but from 2011 onwards, femto-LASIK was more predominant. Supracor and phakic IOL showed a steady rise in numbers during the 5-year study period (Table 2).
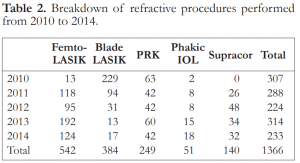
Table 2. Breakdown of refractive procedures performed from 2010 to 2014.
Baseline refractive and visual characteristics
MRSE was highest in the phakic IOL (mean: -9.8D ± 3.44), followed by PRK (-5.07D ± 2.6), and LASIK (mean: -3.77D ± 2.22) groups. Most of the patients had ≤2.00D astigmatism (92%). The Supracor group was hyperopic and presbyopic with a mean uncorrected near visual acuity (UNVA) of J9 (Table 3).

Table 3. Baseline refractive and visual characteristics (N=1366 eyes).
Refractive and visual outcomes at different time points
Sphere
Preoperatively, the mean sphere was -3.32D in the LASIK, -4.66D in the PRK, and -8.96D in the phakic IOL groups. At 1 month follow up, the mean sphere improved to +0.11D in the LASIK, +0.34D in the PRK, and +0.17D in the phakic IOL groups. In the Supracor group, the mean sphere changed from +1.32D preoperatively to -0.46D at one month. In the succeeding follow-up periods, the mean sphere for all groups was maintained (Table 4).

Cylinder
At 1 month follow up, the mean cylinder improved to -0.41D in the LASIK, -0.52D in the PRK, -0.53D in the phakic IOL, and -0.57D in the Supracor groups (Table 4).
Manifest refractive spherical equivalent (MRSE)
After 1 month, the mean MRSE improved from -3.77D to -0.08D in the LASIK, from -5.07D to +0.06D in the PRK, and from -9.8D to -0.11D in the phakic IOL groups. For the Supracor group, the MRSE changed from +1.12D to -0.76D on the 1st month of follow up. The desired MRSE target for Supracor was -0.50D. The succeeding follow-up periods did not show a significant change in MRSE in all groups (Table 4).
Visual acuity
There was a significant improvement in UDVA in the LASIK, PRK and phakic IOL groups. At 1 month postoperatively, the mean UDVA was 20/20 for the LASIK, PRK, and phakic IOL groups and it was maintained at 20/20 even after 2 years. For the Supracor group, the mean UDVA was maintained at 20/30 while the UNVA improved to J1 at 1 month. Mean UDVA and UNVA stayed consistent in all groups up to the 2-year follow up (Table 4).
Refractive outcomes between ≤40 and >40 years old (Myopia)
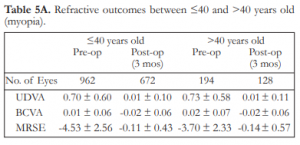
Majority of the myopic patients who had refractive surgery done were ≤40 years old. At 3 months postoperatively, the mean MRSE improved from -4.53D to -0.11D in patients 40 years old and below and from -3.70D to -0.14D in patients above 40 years old. In both groups, preoperative mean UDVA improved from 20/100 to 20/20 (Table 5A).
Table 4. Summary of refractive and visual outcomes at different time points.
Table 5A. Refractive outcomes between ≤40 and >40 years old (myopia).
Refractive outcomes between ≤40 and >40 years old (Hyperopia)
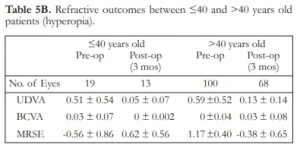
Among the patients with hyperopia who underwent refractive surgery, most belonged to the above 40 year-old age group. At 3 months postoperatively, MRSE improved from -0.56D to +0.62D for those ≤40 years old and from +1.17D to -0.38D for those above 40 years old. In the hyperope ≤40 years old, astigmatism ranged from -1.25D to -6.00D preoperatively and decreased to a range of -0.25D to -1.25D postoperatively. For patients above 40 years old, the cylinder ranged from -0.25D to -5.00D preoperatively and decreased to a range of -0.25D to -1.00D postoperatively. The mean UDVA for patients ≤40 years old improved from 20/63 to 20/20, while for patients above 40 years old it improved from 20/80 to 20/25 (Table 5B).
Table 5B. Refractive outcomes between ≤40 and >40 years old patients (hyperopia).
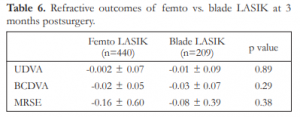
Refractive outcomes of femto vs. blade LASIK at 3 months postsurgery
At 3 months postoperatively, the mean UDVA of both femto and blade LASIK was 20/16. Their mean MRSE were not statistically different with -0.16D for the femto and -0.08D for the blade LASIK groups (p=0.375) (Table 6).
Table 6. Refractive outcomes of femto vs. blade LASIK at 3 months postsurgery.
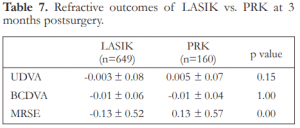
Refractive outcomes of LASIK vs. PRK at 3 months postsurgery
At 3 months postoperatively, the mean UDVA was 20/16 for the LASIK and 20/20 for the PRK. The mean MRSE was -0.13D for the LASIK and +0.13D for the PRK (Table 7).
Table 7. Refractive outcomes of LASIK vs. PRK at 3 months postsurgery.
Complications
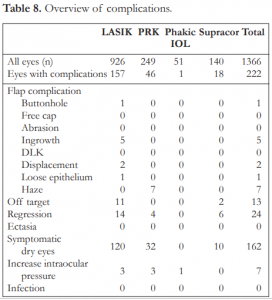
A total of 222 out of 1,366 eyes (16.3%) had various types of complications within the 5-year time frame (Table 8).
Majority (73%) of the complications reported were due to symptomatic dry eye. This comprised 13% of the total LASIK population. Dry eye was considered symptomatic if the patient complained of significant discomfort, poor vision, and had clinical findings of punctate keratitis on slit-lamp examination. Patients were given a combined therapy of sodium hyaluronate eyedrops, lubricating eye gel, and topical cyclosporine (Restasis, Allergan, USA). Two patients had punctal plugs inserted. No patient lost lines of vision in the dry eye group. All patients reported gradual improvement with none reporting significant discomfort by the 6-month follow up. We considered dry eye as a mild, temporary complication with very good prognosis for resolution.
Epithelial ingrowth occurred in 5 cases (0.5%) of LASIK-treated patients (Table 8). In 3 cases, a microkeratome blade was used in flap creation. All but one case underwent a flap lift with ingrowth debridement. No recurrence was reported and no long-term sequalae were noted.
Increased intraocular pressure was reported within the first month postoperatively in 3 cases (0.3%) of LASIK, 3 (1.2%) cases of PRK, and 1 (2%) case of phakic IOL (Table 8). No angle closure was observed on gonioscopy. All cases were considered steroid-induced ocular hypertension. Steroid eyedrops were discontinued and patients treated with brimonidine + timolol (Combigan, Allergan, USA) eyedrops. All cases of increased intraocular pressure resolved within 2 weeks. There were no cases of uncontrolled glaucoma or optic nerve damage reported.
LASIK surgery was aborted in one eye (0.1%) due to buttonhole during the blade microkeratome pass. The BCVA recovered to 20/20 after 3 months. Stromal haze grade 1-2 was observed in 7 cases (2.8%) of PRK-treated eyes. Prednisolone acetate 4 times daily was continued for 3 months. The haze lessened to trace in these eyes with no effect on visual acuity. No incidence of free flap, ectasia, diffuse lamellar keratitis (DLK), abrasion, and infection were reported over the 5-year period in any of the groups (Table 8).
Table 8. Overview of complications.
Enhancement
Reasons for enhancement were divided into regression and off-target (overcorrection and undercorrection) outcomes. After primary PRK, 4 (1.6%) eyes were diagnosed with regression but no case underwent an enhancement procedure. In the LASIK group, 14 (1.5%) eyes had regression and 11 (1.2%) had off-target refractions (Table 8). Eight cases of regression and all 11 cases of off-target outcomes underwent enhancement. In the Supracor group, all 6 (4.3%) cases of regression and 2 (1.4%) off-target outcomes underwent enhancement (Table 9). The mean time from primary surgery to enhancement was 9.4 months for myopic LASIK, 9.6 months for hyperopic LASIK, and 23.5 months for Supracor (Table 9).
Table 9. Enhancement and refractive outcomes 1 month post-enhancement.

DISCUSSION
Refractive screening is performed to determine whether a patient is qualified for refractive surgery, to ascertain which type of surgery is suitable, and to obtain measurements needed for treatment calculation. Among the tests done during refractive screening, the most critical are manifest refraction, corneal thickness, and corneal curvature.
We use the Zyoptix Treatment Calculator (Bausch and Lomb, USA) in computing the amount of corneal tissue to be ablated per diopter of refractive error. To qualify for LASIK, the criteria are residual stromal bed thickness under the corneal flap of at least 280 microns and normal corneal curvature on topography. If unqualified for LASIK, but the residual stromal bed thickness without a flap is computed to be at least 330 microns, PRK is recommended. If the corneal thickness is not enough for LASIK or PRK, but the anterior chamber depth excluding the corneal thickness is at least 2.8 mm, then phakic IOL is the suggested procedure.
LASIK is our first preference because the results are predictable and the procedure is quick and painless. Patients who undergo PRK will have to endure a few days of pain and discomfort and delayed visual recovery. Many patients with thick corneas and normal topographies may be qualified for all three procedures-LASIK, PRK, and phakic IOLs. However, we recommend phakic IOLs as a last option because of the significant price difference, even though phakic IOLs have the advantages of leaving the cornea untouched and having the widest range of refractive correction from +6.0D to -20.0D. Supracor (Bausch and Lomb, USA) is a presbyopic LASIK algorithm wherein we can correct refractive error, astigmatism, and presbyopia simultaneously. This option was discussed with patients above 40 years old who wished to lessen their dependence on reading glasses after their refractive error was corrected.
We embarked on this 5-year review to assess the quality of outcomes of refractive procedures performed in our institution. When patients come and seek a solution to their refractive error, there is a wide spectrum of options available. We needed a periodic evaluation of the procedures we performed so we could recommend a safe and effective treatment with minimal chance of complications for each particular clinical situation.
Approximately 2/3 of all refractive procedures in our institution were LASIK. For over 10 years, we had been using a microkeratome to cut the LASIK flap. In 2010, we began to offer a femtosecond laser option to cut the flap because of its advantage of consistent flap thickness and reduced flap complications, such as buttonholes and free caps. Improved outcomes with regards to vision, induced astigmatism, induced higher-order aberrations, and enhancement rates are seen to favor femtosecond technology over the microkeratome. Recent biomechanical studies also showed improved healing with femtosecond laser flap creation compared with blade-assisted flap creation.9 The femtosecond laser increased the confidence level of both patient and surgeon in LASIK but it carried the burden of additional cost to the patient; so we were not sure of its acceptance when we started. Over the years, we saw a rapid shift wherein patients chose the femtosecond laser for flap creation. Our previous study showed that the refractive and visual outcomes of LASIK were similar between femtosecond laser-created versus microkeratome-created LASIK flaps.10 This was consistent with our findings in this paper wherein the outcomes were similar.
Approximately 20% of patients did not qualify for LASIK and underwent PRK. When excimer-laser refractive surgery first started, everybody underwent PRK because there was no flap technology. Over the years, the census of PRK decreased and LASIK took over because LASIK flaps made refractive surgery quick and painless with rapid visual recovery. However, PRK still has a place in our spectrum of choices because not all patients would qualify for LASIK. We analyzed our data and they showed that refractive and visual outcomes were comparable between LASIK and PRK. Although improvement in uncorrected visual acuity was more rapid in LASIK than in PRK, efficacy outcomes in the longer term generally were similar between the two procedures.11 It is important to validate that PRK outcomes are similar to LASIK so patients do not have the impression that they are being made to undergo an inferior procedure just because they did not qualify for LASIK.
In the past 5 years, phakic IOL was the least performed procedure because the cost was prohibitive. We offered phakic IOL to patients who were not qualified for LASIK or PRK or to those who had spherical equivalent refractive errors beyond -8.0D to spare them from excessive removal of corneal tissue. These eyes were more challenging because they had higher refractive errors but the results showed that the procedure was highly effective and safe. A study by Tsiklis reported that phakic IOL even had better quality of vision, stability, and satisfaction than LASIK.12 Endothelial cell loss was minimal, intraocular pressures were well-controlled, and we have had no explantations so far.
Having a presbyopic LASIK procedure has opened a new market because, previously, these patients had to choose between full correction LASIK with full-time reading glasses or classic monovision wherein the non-dominant eye was targeted to -1.50D. Classic monovision entails sacrificing distance vision to approximately 20/100 to be able to read small print and patients have to endure anisometropia and depth perception issues. Supracor is performed in the non-dominant eye as a modified monovision LASIK strategy. In this study, the mean MRSE was -0.60D at 3 months postoperative, giving the patients a mean UDVA of 20/30 and a mean UNVA of J1. The fellow dominant eye undergoes standard LASIK targeted to maximize full distance correction. This modified monovision combination has allowed us to offer a reliable presbyopic solution to patients above 40 years of age without sacrificing distance vision and inducing profound anisometropia.
An important aspect of safety is the number of complications encountered with each type of refractive procedure. Flap-related problems are unique to LASIK, flap buttonhole being the most significant. In our 5-year review, we encountered only one incident of flap buttonhole while using the blade microkeratome. The procedure was aborted, the flap allowed to heal, and the best-corrected vision returned to 20/20 with no permanent loss of vision. This incident reinforces our belief that femtosecond laser is the ideal device for flap creation. Santhiago and colleagues reported that the incidence of complications, such as epithelial defect and flap dislocation, were higher with microkeratome flaps but we did not encounter these complications in our patient pool.13 There was no incidence of ectasia or corneal weakening. Given that LASIK and PRK reduce corneal thickness, having no ectasia suggests that our screening methods with regard to corneal thickness and curvature are robust and sensitive in avoiding this devastating complication.
Dry eye remains the most common sequelae of refractive surgery. This was predominantly seen in LASIK patients but some PRK patients, likewise, complained of dry eye. Xia and associates observed that the tear-break-up time (TBUT) of LASIK-treated eyes were reduced at 1 week, 1 and 3 months after surgery relative to their preoperative scores, and returned to the preoperative TBUT values at 6 months.14 The reasons for dry eye are multifactorial. First, when flaps are cut during LASIK, corneal nerves that signal basal tear secretion are severed and it takes several months for this lacrimal arc reflex to recover. Second, patients who had many years of contact lens wear have decreased goblet cells resulting in less mucin production, and affecting the tear film layer. Third, a change in corneal curvature after laser refractive surgery may alter the efficient spread of the tear film over the cornea. We routinely prescribe ocular lubricants after refractive surgery to lessen the dry eye discomfort. In our study, we considered dry eye cases that needed more intervention, such as gels, cyclosporine, or punctual plugs as complications. Some would argue that dry eye is not considered a complication because its effects are temporary, more centered on discomfort, and has little bearing on final visual results. However, symptomatic relief of dry eye is crucial because it can affect patient satisfaction, especially during the recovery period when patients are observant and critical of their outcomes.
The goal of refractive surgery is to achieve a refractive correction that is accurate and long term. At times, results may not be optimal because of inaccurate preoperative measurements, variations in laser-tissue interaction, and healing differences between eyes. We define over- and under-correction as unsatisfactory vision due to an off-target refractive outcome, usually above -0.75D of sphere, cylinder or spherical equivalent within the first month of surgery. Regression is defined as an increase in refractive error beyond one month of surgery resulting in unsatisfactory vision. An enhancement procedure (additional excimer laser treatment) is performed to remedy off-target outcomes or regression. However, patients are screened first for adequacy of corneal tissue. Our enhancement rate for LASIK was 2.1% over a 5-year review of data whereas other studies reported enhancement rates of 6.85% (Mexico)15 over a 3-year review and 3.8% (Singapore)1 over a 10-year review of outcomes. Our enhancement rate was low and comparable with other studies, suggesting that our nomograms and protocols were accurate in refractive correction. Supracor has a 6% enhancement rate due to regression. We attributed this to two factors. First, presbyopia continues to progress over time; therefore, the gain in near vision may naturally wane over time. Second, being a relatively new algorithm, we need to fine-tune the Supracor calculation to adjust and account for regression of hyperopic LASIK and increasing presbyopia with time.
Our 5-year retrospective study of 1,366 eyes highlighted several trends and reinforced several known findings. Femtosecond laser-created flaps have become the norm in LASIK. PRK procedures are still performed. Phakic IOLs are important in addressing the high refractive error population and those who do not qualify for LASIK or PRK. Presbyopic LASIK treatments are increasing. Complication and enhancement rates of refractive surgery are low. Refractive surgery procedures continue to be safe, effective, and predictable.
REFERENCES
1. Yeun LH, Chan WK, Koh J, et al, SingLasik Research Group. A 10-year prospective audit of LASIK outcomes for myopia in 37,932 eyes at a single institution in Asia. Ophthalmology 2010;117:1236-1244.
2. Solomon KD, Fernández de Castro LE, Sandoval HP, et al, Joint LASIK Study Task Force. LASIK world literature review: quality of life and patient satisfaction. Ophthalmology 2009;116:691-701.
3. Alió JL, Soria F, Abbouda A, et al. Laser-in-situ keratomileusis for -6.00 to -18.00 diopters of myopia and up to -5.00 diopters of astigmatism: 15-year follow up. J Cataract Refract Surg 2015;41:33-40.
4. Alió JL, Ortiz D, Muftuoglu O, et al. Ten years after photorefractive keratectomy (PRK) and laser-in-situ keratomileusis (LASIK) for moderate to high myopia (control-matched study). Br J Ophthalmol 2009;93:1313-1318.
5. Shalchi Z, O’Brart DP, McDonald RJ, et al. Eighteen-year follow up of excimer laser photorefractive keratectomy. J Cataract Refract Surg 2015;41:23-32.
6. American Academy of Ophthalmology Refractive Management/Intervention. Preferred Practice Pattern Guidelines. Refractive Errors & Refractive Surgery. San Francisco, CA: American Academy of Ophthalmology, 2013. Available at: www.aao.org/ppp.
7. Ryan A, O’Keefe M. Corneal approach to hyperopic presbyopia treatment: six-month outcomes of a new multifocal excimer laser-in-situ keratomileusis procedure. J Cataract Refract Surg 2013;39:1226-1233.
8. Saib N, Abrieu-Lacaille M, Berguiga M, et al. Central PresbyLASIK for hyperopia and presbyopia using micro-monovision with the Technolas 217P platform and SUPRACOR algorithm. J Refract Surg 2015;31:540-546.
9. Stonecipher K, Ignacio TS, Stonecipher M. Advances in refractive surgery: microkeratome and femtosecond laser flap creation in relation to safety, efficacy, predictability, and biomechanical stability. Curr Opin Ophthalmol 2006;17:368-72.
10. Perez RC, Cruz EM, Dela Cruz Jr AG, et al. Comparison of flap thickness, visual outcomes, and higher-order aberrations in eyes that underwent LASIK flap creation using a femtosecond laser versus a mechanical microkeratome. Philipp J Ophthalmol 2012;37:83-90.
11. Hersh PS, Brint SF, Maloney RK, et al. Photorefractive keratectomy versus laser-in-situ keratomileusis for moderate to high myopia: A randomized prospective study. Ophthalmology 1998;105:1512–1523.
12. Tsiklis NS, Kymionis GD, Karp CL, et al. Nine-year follow up of a posterior chamber phakic IOL in one eye and LASIK in the fellow eye of the same patient. J Refract Surg 2007;23:935-7.
13. Santhiago MR, Kara-Junior N, Waring GO. Microkeratome versus femtosecond flaps: accuracy and complications. Curr Opin Ophthalmol 2014;25:270-274.
14. Xia LK, Yu J, Chai GR, et al. Comparison of the femtosecond laser and mechanical microkeratome for flap cutting in LASIK. Int J Ophthalmol 2015;8:784-790.
15. Valdez-García JE, Hernandez-Camarena JC, Martínez-Muñoz R. 3-Year follow up after LASIK: assessing the risk factors for retreatment. Int Ophthalmol 2015.