Treatment Outcomes of Retinoblastoma Patients at a Tertiary Government Hospital in the Philippines
Jayson T. So MD DPBO, Fatima G. Regala MD DPBO, Beltran Alexis A. Aclan MD DPBO
Department of Health Eye Center, East Avenue Medical Center, Quezon City
Correspondence: Jayson T. So MD DPBO
Office Address: Department of Health Eye Center, East Avenue Medical Center, East Avenue, Diliman, Quezon City, Philippines
Clinic phone number:+632-8928-0611
Email Address: jaysontso1@gmail.com
Disclosure: The authors report no financial interests.
Retinoblastoma (RB) is the most common intraocular malignancy among children. It is both vision- and life-threatening. Early diagnosis and treatment are important to save life, maintain useful vision, and allow for better cosmesis and quality of life. Delay in management can lead to the rapid progression of the disease, causing loss of vision, loss of the eye, poor cosmesis, metastasis, and death. The National Retinoblastoma Strategy – Canadian Guidelines for Care reported that majority of children diagnosed with retinoblastoma are cured given that timely screening, diagnosis, referral, treatment, and follow-up are delivered by a multidisciplinary team.1
In the 21st century, treatment of retinoblastoma has evolved to involve a wide-range of modalities from enucleation to globe-preserving techniques such as administration of systemic chemotherapy, intra-arterial chemotherapy, ruthenium-106 plaque brachytherapy, external beam radiation therapy, cryotherapy, transpupillary thermotherapy, subtenon chemotherapy, and intravitreal chemotherapy.2 Outcomes are generally successful for the early stages of disease with reported overall 5-year survival rate at 93.8%.2 However, despite new advances in globe-preserving treatment of retinoblastoma, enucleation still remains to be the treatment of choice in advanced disease.
Measures of treatment outcomes include rates of globe preservation, disease-free survival and 5-year survival.3 There are few epidemiological studies on retinoblastoma cases in the Philippines. More so, local data on treatment outcomes are scarce. A recent paper reported overall 2-year survival rate of 53% among retinoblastoma patients treated in a tertiary hospital in the northern Philippines while survival outcome was only known in 39% retinoblastoma patients seen in a government hospital in the Philippine capital with two-thirds of this number succumbing to the disease. 4,5
The objective of this study was to describe the clinical outcomes of patients with retinoblastoma seen at a tertiary government hospital in the Philippines from January 2000 to January 2020.
METHODS
This study employed a retrospective cohort design. Medical records of all patients with histology-proven retinoblastoma seen at the East Avenue Medical Center from January 2000 to January 2022 were reviewed. The census of patients was derived from the Department of Ophthalmology of the hospital. Patients with histology-proven retinoblastoma were included in the study. Patients who were clinically diagnosed with retinoblastoma without histopathologic confirmation were excluded. Data collection was carried out from November 2021 to January 2022.
The following data from the medical charts were recorded: age, sex, laterality, age at symptom onset, age at initial consult, age at treatment initiation, initial presenting symptom, family history of retinoblastoma, International Classification of Retinoblastoma (ICRB) grade, treatment received, and the presence of high-risk features.
The primary study outcomes were globe preservation, and 3- and 5-year overall survival rate. Globe preservation is defined as absence of recurrence using globe salvage strategies. Globe salvage strategies is defined as treatment free from enucleation or exenteration. Overall 5-year survival rate is defined as the percentage of patients who are alive 5 years after diagnosis.
This study was approved by the East Avenue Medical Center Institutional Ethics Review Board and was conducted in accordance to the Declaration of Helsinki.
Statistical analyses
Demographic data was reported using descriptive statistics. The Kaplan-Meier method was used to estimate overall survival. The log-rank test was used to explore how clinical characteristics such as ICRB staging and laterality affect survival curves. Univariate Cox regression analysis was used to calculate hazard ratios. Data from all evaluable subjects were included in the analysis. Missing values were not replaced or estimated during the analysis. Patients who were lost to follow-up were still included in the study using their last known follow- up. All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) version 24. For all analyses, level of statistical significance was set at 0.05.
RESULTS
A total of 118 patients (146 eyes) were included in this study. Males accounted for 49% of the study patients (n=58) (Table 1). The mean age at symptom onset was 7.4 + 6.6 months (range 0.2-24). Meanwhile, the mean age at diagnosis was 12.3 + 9.8 months (range 1.5-49). Majority of the patients (n=90 or 76.3%) had unilateral disease. The mean age of symptom onset was similar for patients with unilateral and bilateral disease (7.71 vs. 7.32 months, p>0.05). Only one patient (0.8%) had a positive history of familial retinoblastoma. The most common presenting symptoms were leukocoria (80.5%), proptosis (17.8%), and swelling (14.4%).
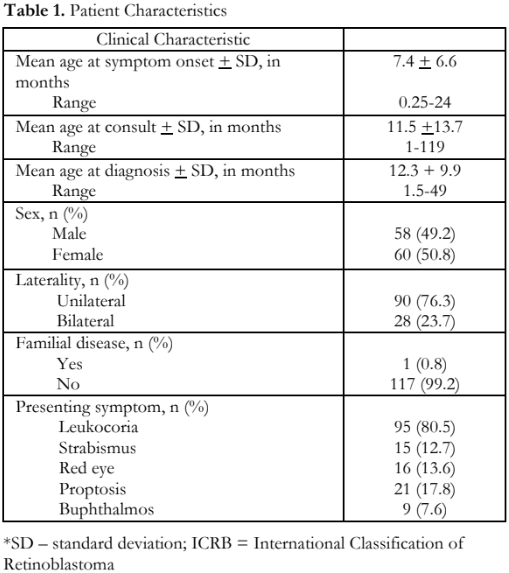
Of the 146 eyes, 3 (2.1%), 2 (1.4%), 8 (5.5%), 24 (16.4%), 69 (47.3%), and 33 (22.6%) were classified under ICRB groups A, B, C, D, E, and EO, respectively (Figure 1). For patients with unilateral retinoblastoma (n=90 eyes), 47 (52%) had stage ICRB E disease. For patients with bilateral retinoblastoma (n=56 eyes), 22 (39.3%), and 19 (33.9%) had stage ICRB E and EO disease, respectively.
Of the 146 eyes, 137 (93.8%) were primarily treated with enucleation, 4 (2.7%) with exenteration, and 5 (3.4%) with laser photocoagulation. Two eyes from patients with bilateral retinoblastoma were initially treated with laser photocoagulation as globe salvage therapy, but these eventually underwent secondary enucleation due to disease progression. In this study, there were 3 (2.5%) patients who received neoadjuvant chemotherapy while 59 (50%) received adjuvant chemotherapy.
High-risk histopathologic features were present in 39 (27.3%) out of 143 eyes that had either primary or secondary enucleation or exenteration. The most common high risk histopathologic features were involvement of the optic nerve (19.9%), followed by the choroid (9.6%), anterior chamber (8.9%), sclera (8.2%), ciliary body (6.8%), and iris (4.8%).
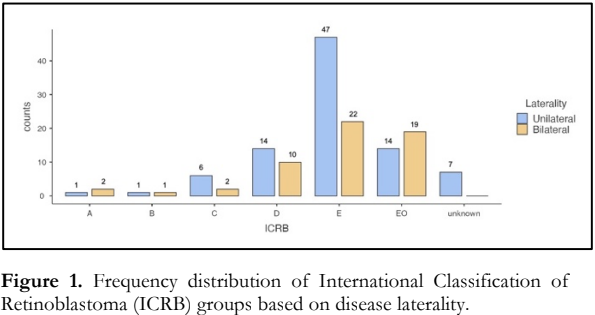
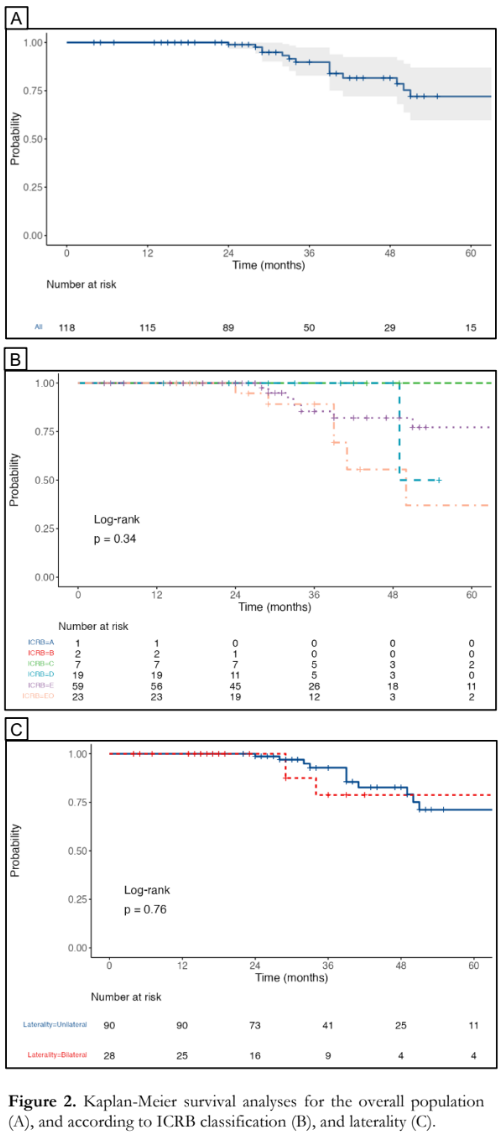
Median follow-up was 30.5 months (1st and 3rd interquartile range= 24, 48). Kaplan-Meier analysis for the overall population showed an overall survival of 100%, 89.8% (95% CI 82.8-97.4%) and 72% (95%CI 59.7-87%) at 2, 3 and 5 years, respectively [Figure 2A]. On log rank tests, there were no significant differences in survival among the different ICRB classifications (p=0.34) [Figure 2B] and between unilateral and bilateral disease (p=0.76) [Figure 2C].
On univariate Cox regression analysis, patients who initially presented with proptosis and buphthalmos had significantly higher risk of death, with hazard ratios of 6.84 (95%CI 2.02-23.12, p=0.002) and 5.56 (95%CI 1.73-17.80, p=0.004), respectively (Table 2).

DISCUSSION
Epidemiological studies on retinoblastoma, particularly on treatment and outcomes, are relatively scarce in developing countries like the Philippines. This study presented data from a national referral center located in the National Capital Region. The overall age of symptom onset at our institution is lower at 7.4 months compared to other local papers with 14 months. However, this is subject to recall bias as primary care givers may have different interpretations of symptoms. Closer data to local studies is the age of consult at 11. 54 months. Our data also showed that among those diagnosed with retinoblastoma, there was equal distribution of females and males. These findings are comparable with other locally and internationally published studies showing that there is no sexual predilection among patients diagnosed with the disease.4-8 There is a lower familial incidence noted in our data at 1% compared to another local study showing 7%.6 Consistent with other published data, the most common presentations was leukocoria followed by proptosis, strabismus, orbital swelling and red eye.4,5,6,7,9 In terms of clinical staging, our study revealed a high percentage of patients with extraocular involvement at 33 (22.6%) and ICRB Group E at 69 (47.3%) showing that most patients presented with more advanced stage of disease similar with local and international data sharing the same demographic.5,7,8 This may be due to several contributory factors that are already beyond the scope of this study.
In this study, similar with majority of published data in low-medium income countries, enucleation comprises majority of the treatment modality for advanced stages of the disease.5,9 Despite new advances in globe-preserving treatment of retinoblastoma, enucleation still remains to be the treatment of choice in advanced retinoblastoma.10 Exenteration is rare in current practice, but in this study 2.7% of patients still underwent the procedure for extraocular involvement in the past two decades. Moreover, only 50% of patients underwent chemotherapy post-enucleation. Eyes with IRCB Group E disease are generally considered unsalvageable and pose significant risk to life; therefore enucleation is warranted as the primary treatment. Of the 28 patients with bilateral involvement, only 8 patients had a lower clinical ICRB staging (A-B) on the better eye allowing the use of laser photocoagulation. However, 2 progressed prompting enucleation. Three patients received neoadjuvant chemotherapy and belonged to stage E with extraocular spread. Involvement of the optic nerve at the cut end was the most common high risk feature. Due to limited data and follow up, rates of globe salvage cannot be determined.
Survival rate was higher in our study at 100% at 2 years compared to another local study that reported a survival rate of 57% at 2 years for retinoblastoma patients seen at a tertiary hospital in Northern Luzon. This may be due to differences in patient socioeconomic status and accessibility to health care.4 Furthermore, our data showed that overall survival starts to decrease at 3 years of age, dropping to 72% at the age of 5. This data is comparable to retinoblastoma patients from India, which has similar demography to the Philippines, with an overall survival rate of 75%.11 Patients presenting with proptosis and buphthalmos had a lower chance of survival contributing to the lower overall survival of the patients in this institution. Other factors that may worsen the baseline prognosis include a higher stage at presentation, longer diagnostic time, and poorer follow up practices.12
The present study described the clinical outcomes in terms of overall survival rate in relation to selected clinical features of patients that were diagnosed and treated at a national eye referral center in the Philippines. The profile of our patients were comparable to published data from different developing countries. Also, the diagnosis of retinoblastoma in our setting occurred at a relatively advanced clinical stage of the disease.
There are several limitations to this study. Firstly, the relatively small sample size because of it being a single-centered study as compared to other epidemiological studies done in other countries. Secondly, because the study uses a retrospective study design, selection bias is inherent. Lastly, survival analysis may be limited due to poor patient follow up.
Retinoblastoma and its serious consequences are important. There are few centers such as the Department of Health Eye Center (DOH EC) that are developing their own retinoblastoma registry.
However, to generate data reflective of the general population, the establishment of a nationwide retinoblastoma registry is necessary. This will allow proper surveillance of cases, monitoring of outcomes and generation of multi-centered studies. From this, we suggest that all tertiary government hospitals be equipped with proper facilities to handle such cases to expedite management and prevent mortality and morbidity from the disease.
REFERENCES
- Canadian Retinoblastoma Society. National Retinoblastoma Strategy Canadian Guidelines for Care: Stratégie thérapeutique du rétinoblastome guide clinique canadien. Can J Ophthalmol. 2009;44 Suppl 2:S1-88..
- Rojanaporn D, Attaseth T, Dieosuthichat W, et al. Clinical presentations and outcomes of retinoblastoma patients in relation to the advent of new multimodal treatments: A 12- Year report from single tertiary referral institute in Thailand. Journal of Ophthalmology. 2020;1-13.
- Gündüz AK, Mirzayev I, Temel E, et al. (2020). A 20-year audit of retinoblastoma treatment outcomes. Eye. 2020;34(10):1916-1924.
- Tan RJD, Ballesteros KFB. Retinoblastoma Outcomes in a Tertiary Hospital in Northern Luzon, The Philippines: A 15-Year Experience. South Asian J Cancer. 2022;11(2):160- 163.
- Torno MM, Tan MF, Facundo AR, et al. A 10-Year Retrospective Study on the Presentation, Treatment, and Outcomes of Retinoblastoma Patients in a Philippine Tertiary Hospital. Philipp J Ophthalmol. 2023:48;10-15.
- Espiritu RB, de Jesus AA, Valera EG, Mercado GV. Epidemiological Pattern of Retinoblastoma at the Philippine General Hospital Philipp J Ophthalmol 2004;29:136-139
- Noguera SI, Mercado GV, Santiago DE. Clinical epidemiology of retinoblastoma at the Philippine General Hospital: 1998-2008. Philipp J Ophthalmol. 2011;36(1):28-32.
- Li SY, Chen SCC, Tsai CF, et al. Incidence and survival of retinoblastoma in Taiwan: a nationwide population-based study 1998 −2011. Br J Ophthalmol. 2016;100:839–842.
- Kaliki S, Srinivasan V, Gupta A, et al. Clinical Features Predictive of High-Risk Retinoblastoma in 403 Asian Indian Patients. Ophthalmology. 2015;122(6):1165–1172.
- Zhao J, Feng ZX, Wei M et al. Impact of Systemic Chemotherapy and Delayed Enucleation on Survival of Children with Advanced Intraocular Retinoblastoma. Ophthalmol Retina. 2020;4(6):630-639.
- Tan RD. Clinical presentation, treatment, and outcomes of retinoblastoma in India: A literature review. Philipp J Health Research Dev. 2022;26(61-72):61-72.
- Chantada GL, Qaddoumi I, Canturk S, et al. Strategies to manage retinoblastoma in developing countries. Pediatr Blood Cancer. 2011;56:341–8.