Retinal Nerve Fiber Layer Measurements in Myopia Using Optical Coherence Tomography
Dennis L. del Rosario, MD and Mario M. Yatco, MD
Myopia is a common ocular abnormality worldwide with a prevalence in adults of 22.7% and 26.2%, reported in the Baltimore Eye Survey and theBeaver Dam Study, respectively.1–2 Among adult Chinese in Singapore, it was estimated that 38.7% of adult Chinese were myopic and 9.1% were high myopes.3 From the clinical and socioeconomic standpoints, these are major concerns especially among East Asian countries where there are projections for increasing prevalence rate and severity of the condition.4 One of the potentially blinding ocular diseases found to have a strong relationship with myopia is glaucoma5 which is characterized by progressive degeneration of retinal ganglion cells, one of the common ocular diseases seen among Filipinos. An important approach in the detection of early structural change in glaucoma is based on assessment of the retinal nerve fiber layer (RNFL) using the optical coherence tomography (OCT). Numerous studies have confirmed that RNFL measurement is sensitive in detecting glaucoma, and the extent of RNFL damage correlates with the severity of functional deficits in the visual field.6–8 Some patients can lose up to 40% of their RNFL before any visual field defect is detected. The Stratus OCT utilizes a normal population database for RNFL measurements, developed by the manufacturer and packaged within the software. However, it did not include individuals with moderate or high degrees of myopia and there were only 11 Asians out of the 328 subjects included in the establishment of the normative reference values for RNFL thickness measurement.9 RNFL thinning is indicative of glaucomatous damage; however, it remains uncertain whether RNFL thickness would vary with the degree of myopia where eyes have longer axial lengths and stretched-out retina. Conflicting data existed regarding the influence of myopia on peripapillary retinal nerve fiber layer (RNFL) thickness. Some studies showed no association whereas others found significant correlations.9 This study investigated if there is a significant relationship between the degree of myopia and RNFL thickness as measured by optical coherence tomography.
METHODOLOGY
Adult Filipinos, between 18-39 years of age, with myopia of ≥0.75 D and no ocular or systemic conditions that can affect the refraction , were recruited from July 2012 to August 2012 at the outpatient department of the Department of Ophthalmology, University of Santo Thomas Hospital. Subjects less than 18 years old, spherical equivalent <-0.75 D, diagnosed glaucoma or glaucoma suspect with CD ratio ≥0.5, those with frank presbyopia, and those with ocular diseases such as cataract and any form of retinopathy were excluded.
All subjects underwent complete ophthalmologic examination consisting of visual acuity determination, refraction, applanation tonometry, slit lamp evaluation, stereoscopic biomicroscopy of the optic nerve head at the slit lamp using a 90 D lens, and fundoscopy. OCT was performed with the Stratus OCT (Carl Zeiss, Meditec Inc.). RNFL thickness was measured with the fast RNFL scanning protocol (256 A-scans). Average measurements of three sequential circular scans with a diameter of 3.4 mm centered on the optic disc were recorded. All the scans had signal strength of at least 7. Parameters including average RNFL thickness and mean RNFL thickness in each quadrant were generated automatically in the analysis report of the Stratus OCT. Correlations between refraction (spherical equivalent) and RNFL thicknesses were determined by linear regression analysis and expressed as the Pearson coefficient of correlation (r), with p<0.05 considered statistically significant.
RESULTS
Twenty-eight eyes of 14 myopic subjects were included in the study. The mean age and spherical
equivalent were 25 years (range, 22–35) and -3.50 D (range, -0.75 to -6.00), respectively. The average RNFL thickness in myopic eyes with -0.75 D to -3.00 D was 102.44 µm (range, 91.65 to 116.28 μm) and in myopic eyes with >-3.00 D 97.91 µm (range,77.67 to 117.51 μm). A significant proportion of myopic eyes (78%) were classified as below normal limits, with reference to the normative database of the retinal nerve fiber layer measurement of the Stratus OCT (Table 1).

There was a significant correlation between refraction and average RNFL thickness (p=0.036) (Figure 1). For every 1.00 D decrease in refraction (more myopic), there was a 2.868 µm decrease in the average RNFL thickness (Table 2).

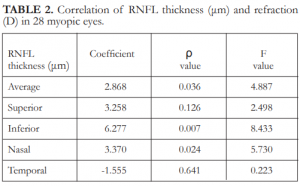
There was, however, no significant correlation between the refraction and the superior and temporal RNFL thickness (p = 0.13 and 0.64, respectively) (Figures 2 and 3; Table 2).

Figure 2. Refraction (SE) and superior RNFL thickness (µm) in 28 myopic eyes.
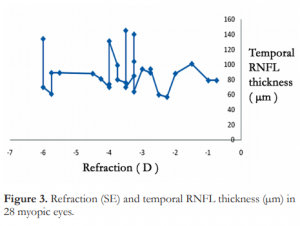

Figure 6. Representative retinal nerve fiber layer scans from normal subjects with different degrees of myopia.
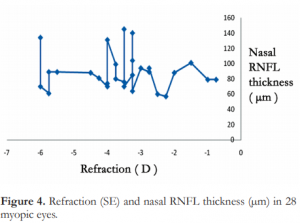
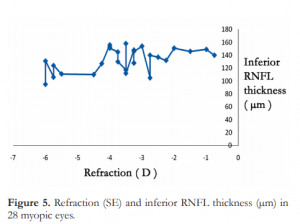
The most frequently abnormal sector was at the nasal quadrant, where 78% of the myopic eyes were below normal limits. A significant correlation was seen between refraction and nasal RNFL thickness (p=0.02). There was a corresponding decrease of 3.37 µm in the nasal RNFL thickness for every 1.00 D decrease in refraction (more myopic) (Figure 4 and Table 2). There was also a significant correlation between refraction and inferior RNFL thickness (p=0.007). For every decrease of 1.00 D in refraction (more myopic), there was a decrease of 6.278 µm in the inferior RNFL thickness (Figure 5 and Table 2). Representative RNFL scans of the different
degrees of myopia are shown in Figure 6.
DISCUSSION
Our findings indicated that the average retinal nerve fiber layer thickness decreases as the refraction becomes more myopic. These data supported the findings of Schweitzer10 and Leung11 that there is a positive correlation between refraction and RNFL thickness. This is in contrast to the results found by Hoh12 where the mean RNFL thickness did not vary with the degree of myopia when investigated by OCT. In our study, we found that there was a decrease in the RNFL thickness at the nasal quadrant, 78% of which were below normal limits based on the normative database of the Stratus OCT. A positive correlation between the degree of myopia and the
nasal RNFL thickness was observed. There was a decrease of 3.37 µm for every 1.00 D decrease in refraction. This data supported the findings of Leung11 that Chinese myopic subjects have thin nasal RNFL, a finding not found in the largely Caucasian population where Rauscher noted that thin RNFL in myopic subjects occurred preferentially at the superior and inferior quadrants.9 We also found that there was a positive correlation between the degree of myopia and RNFL thickness at the inferior quadrant but the majority were within normal range and only 3% were below 95%. The Stratus OCT used in this study provided superior image quality and higher resolution scanning of the RNFL compared to earlier models. Although newer generation OCT are now available, the Stratus OCT remains to be widely used in the Philippines. The Stratus OCT provides a database with agematched controls for comparative analysis aiding the detection of ocular diseases involving the RNFL but myopia have been reported.10 Myopic globe elongation may seem to stretch and thin the RNFL because of mechanical forces.11 Myopic retinal degeneration may account for decrease RNFL thickness and a larger disc with normal ganglion cells may provide a greater surface area for axon distribution.13 On the other hand, the decreased RNFL thickness among myopes could represent a predisposing factor for future development of glaucoma that could partly explain the increase incidence among myopes in some studies like the Blue Mountain Eye Study where data showed strong relationship between open-angle glaucoma and myopia.5 In conclusion, RNFL measurements may vary with refraction. There is a decrease in the average RNFL thickness as the refractive error becomes more myopic which may suggest the need for the Stratus OCT RNFL normative database to have corrective factors for refractive error among myopic patients and to verify these data with the use of the new generation Cirrus OCT. Although both nasal and inferior quadrants positively correlate with myopia, majority of the nasal quadrant showed below normal thickness based on the Stratus OCT normative database. A careful interpretation of RNFL measurements, especially the nasal quadrant, should be done among myopic subjects to avoid mislabeling them as glaucoma suspects.
REFERENCES
1. Katz J, Tielsch JM, Sommer A. Prevalence and risk factors for refractive errors in an adult inner city population. Invest Ophthalmol Vis Sci 1997;38:334-340.
2. Wang Q, Klein BE, Klein R, Moss SE. Refractive status in the Beaver Dam Eye Study. Invest Ophthalmol Vis Sci
1994;35:4344-4347.
3. Wong TY, Foster PJ, Hee J, et al. Prevalence and risk factors for refractive errors in adult Chinese in Singapore. Invest Ophthalmol Vis Sci 2000;41:2486-2494.
4. Seet B, Wong TY, Tan DT, et al. Myopia in Singapore: taking a public health approach. Br J Ophthalmol 2001;85:521-526.
5. Mitchell P, Hourihan F, Sandbach J, et al. The relationship between glaucoma and myopia: the Blue Mountains Eye Study. Ophthalmology 1999;106:2010-2015.
6. Leung CK, Chan WM, Yung WH, et al. Comparison of macular and peripapillary measurements for the detection of glaucoma: an optical coherence tomography study. Ophthalmology 2005;112:391–400.
7. Hoffmann EM, Medeiros FA, Sample PA, et al. Relationship between patterns of visual field loss and retinal nerve fiber layer thickness measurements. Am J Ophthalmol 2006;141:463-471. the validity of applying this database to healthy myopes is yet to be verified.11 The study of Rauscher9 pointed out that extremes of refractive error were excluded and the normative database lack the exclusionary criteria based on refractive error. Moreover, there were only 11 Asian eyes out of 328 included in the study establishing the database where majority were whites (205 eyes). Statistical analyses were done between RNFL thickness and age, right vs left eye, and gender, but not the ethnicity. Therefore, it would be of interest to examine whether there is a significant difference in RNFL thickness measurements between Asians and non-Asians. Several explanations for RNFL thinning inn8. Medeiros FA, Zangwill LM, Bowd C, et al. Comparison of the GDx VCC scanning laser polarimeter, HRT II confocal scanning laser ophthalmoscope, and Stratus OCT optical coherence tomography for the detection of glaucoma. Arch Ophthalmol 2004;122:827-837.
9. Rauscher FM, Sekhon N, Feuer WJ, et al. Myopia affects retinal nerve fiber layer measurements as determined by optical coherence tomography. J Glaucoma 2009:18:501-505.
10. Schweitzer KD, Ehmann D, Garcia R. Nerve fibre layer changes in highly myopic eyes by optical coherence tomography. Can J Ophthalmol 2009; 44:13-6.
11. Leung CK, Mohamed S, Leung KS, et al. Retinal nerve fiber layer measurements in myopia: an optical coherence tomography study. Invest Ophthalmol Vis Sci 2006;47:5171– 5176.
12. Hoh ST, Lim MC, Seah SK, et al. Peripapillary retinal nerve fiber layer thickness variations with myopia. Ophthalmology 2006;113:773–777.
13. Kremmer S, Zadow T, Steuhl KP, et al. Scanning laser polarimetry in myopic and hyperopic subjects. Graefes Arch Clin Exp Ophthalmol 2004;242:489–494.