Cholesterol Granuloma as a Rare Differential in Bone Erosion of the Orbit: A Case Report
Mary Rose Pe Yan MD, Gian Carlo Aurelio MD, Felice Katrina T. Ranche MD
Department of Ophthalmology and Visual Sciences, University of the Philippines – Philippine General Hospital, Manila
Correspondence: Mary Rose Pe Yan MD
Clinic Address: Department of Ophthalmology and Visual Sciences, University of the Philippines – Philippine General Hospital
Clinic telephone number: +639175204320
Email address: mlpeyan1@up.edu.ph
Disclosure: The authors report no financial disclosures.
A computed tomography (CT) scan finding of a well-circumscribed mass with extensive bone erosion in the superotemporal orbit is most commonly attributed to a malignant lacrimal gland tumor.1 However, benign orbital lesions, such as cholesterol granuloma, aneurysmal bone cysts, cystic ossifying fibroma, and dermoid cyst, can also present with bone erosion in the area of the lacrimal fossa, making them differential diagnoses of lacrimal gland malignancy.2 Cholesterol granulomas are rare benign lesions that arise most commonly in the bony structures of the cranium. They can be found in the breast, lungs, kidneys, lymph nodes, and peritoneum.3 In the orbit, they are most frequently found in the air spaces of the temporal bone. Bone erosion is a radiologic hallmark of orbitofrontal cholesterol granulomas.4
Herein, we report a case of orbitofrontal cholesterol granuloma as a rare differential diagnosis of orbital erosion in the diploe of the frontal bone.
CASE REPORT
A 50-year-old man presented with displacement of the right eye associated with ptosis, tearing, foreign body sensation, and blurred vision of one-month duration. He was otherwise in good health with no history of facial trauma. The rest of the clinical history was unremarkable. On examination, best-corrected visual acuity was 20/20 in each eye. Grossly, there was a palpable, soft, non-tender, orbital mass on the right superotemporal area, measuring 30 mm in length and 10 mm in height. There was resistance to retrodisplacement of the globe and moderate ptosis on the upper lid with good levator function. The right eye was displaced anteriorly, inferiorly, and medially (Figure 1). Hertel exophthalmometer measurements were 18 mm on the right eye and 12 mm on the left eye, with a base of 102 mm. There was no strabismus in the primary position, but there was slightly limited abduction of the right eye. The intraocular pressure (IOP) was 16 mmHg in both eyes. The anterior segment and fundus examination were normal in both eyes.
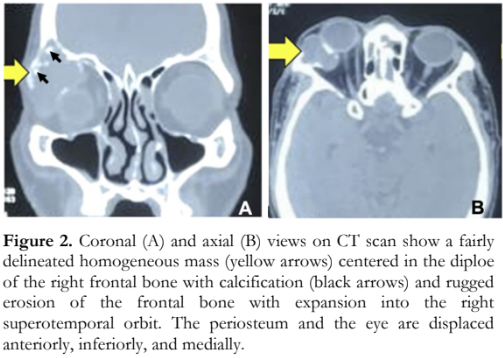
CT scan of the orbit showed a fairly delineated homogeneous mass with calcification centered in the diploe of the right frontal bone and extending into the right superotemporal orbit (Figure 2). There was rugged erosion of the frontal bone. The periosteum and the eye were displaced anteriorly, inferiorly, and medially.

The patient underwent an orbitotomy to excise the mass. Routine histopathologic examination with hematoxylin and eosin stain showed numerous needle-shaped cholesterol clefts surrounded by inflammatory cells, including foreign body giant cells, histiocytes with foamy cytoplasm, and hemosiderin- laden macrophages, and blood degradation products. These histopathologic findings were consistent with cholesterol granuloma (Figure 3).

DISCUSSION
Orbital cholesterol granuloma is a rare soft tissue mass that typically presents on CT scan as a lesion in the superotemporal orbit that is isodense with brain, extends to the extraperiosteal space of the lacrimal fossa, causes bone erosion of the orbital roof with minimal or no sclerosis of the surrounding bone, and causes proptosis and inferior displacement of the globe.5 Bone spiculation may be seen and appears as calcification within the lesion. Cholesterol granulomas do not enhance with contrast. The predilection of orbital cholesterol granuloma for the lacrimal fossa is unknown. However, Chow and McNab reported hemorrhage and the breakdown of blood products to be the source of cholesterol that then crystallizes and causes a granulomatous reaction.6 Metabolic degradation of hemoglobin results in products that give the lesion its characteristic features; that is, hemosiderin deposits give the brownish color, lipid gives the yellowish color, and cholesterol crystals give the glistening property.7 Cholesterol crystals are strong irritants that trigger an irreversible foreign body reaction. In the inflammatory reaction, capillary growth is stimulated, and erythrocytes and inflammatory cells transude to cause continued expansion of the mass.8 The newly-formed pathologic blood vessels have a tendency to rupture to form areas of hemorrhage, resulting in a vicious cycle. As the granuloma expands, it exerts pressure on surrounding tissues and can lead to osteolysis.
The common radiologic differentials for a mass causing irregular bone destruction with or without sclerosis in the superotemporal orbit are dermoid cyst and lacrimal gland malignancy.5 Since the management of lacrimal gland malignancy is more radical, awareness of the possibility of osteolysis due to a benign lesion, like cholesterol granuloma, is important. Orbital cholesterol granuloma is adequately treated with complete removal through simple drainage, curettage, or drilling of the involved bone. On clinical history, malignant lacrimal gland tumors are usually associated with pain, and orbital cholesterol granulomas are usually associated with trauma. However, the absence of pain or trauma cannot exclude these differentials.
The association between orbital cholesterol granuloma and trauma has evolved through the years. When Denig first described cholesterol granuloma of the orbit in 1902, he attributed a 10-year history of trauma to the orbital wall to be the cause of an elastic tumor to develop behind the lacrimal gland, resulting in proptosis and an orbital roof defect.9 In the Philippines, Santiago and Sua reported a similar case of an expansile orbital lesion that presumably arose from incompletely resorbed orbital hemorrhage that resulted from trauma.10 McNab postulated that prominence of the frontal bone and predilection for males were factors that favored trauma as the cause of hemorrhage. Cases that did not report past trauma could be due to mild injury that may have been forgotten. In a systematic review of literature involving 172 cases of orbital cholesterol granuloma, Hughes et al. reported only 21.5% of patients to have a history of recent or remote trauma.11 Parke et al. discussed that due to the relative frequency of periorbital trauma and the relative rarity of orbital cholesterol granuloma, it is highly unlikely that there is an association between trauma and cholesterol granuloma.12 Instead, Parke suggested that an intradiploic anomaly causes the predisposition to the development of a cholesterol granuloma.
Cholesterol granulomas represent an infrequent but important consideration in cases of bone erosion within the orbit. Recognizing their unique features and distinguishing them from other orbital lesions is crucial for accurate diagnosis and appropriate management. This case demonstrates that the presence of bone erosion on radiologic imaging should not exclude the possibility of a benign tumor.
REFERENCES
- Wright JE, Rose GE, Garner A. Primary malignant neoplasms of the lacrimal gland. Br J Ophthalmol. 1992;76(7):401-7.
- Yan J, Cai Y, Liu R, et al. Cholesterol granuloma of the orbit. J Craniofac Surg. 2015;26(2):e124-6.
- Aferzon M, Millman B, O’Donnell TR, Gilroy PA. Cholesterol granuloma of the frontal bone. Otolaryngol Head Neck Surg. 2002;127(6):578-81.
- Rong AJ, Erickson BP, Blessing NW, et al. Orbital cholesterol granuloma: A report and discussion of orbital findings. Am J Ophthalmol Case Rep. 2019 May;15:100468.
- Hill CA, Moseley IF. Imaging of orbitofrontal cholesterol granuloma. Clin Radiol. 1992 Oct;46(4):237-42.
- Chow LP, McNab AA. Orbitofrontal cholesterol granuloma. J Clin Neurosci. 2005 Feb;12(2):206-9.
- Nager GT, Vanderveen TS. Cholesterol Granuloma Involving the Temporal Bone. Annals Otol Rhinol Laryngol. 1976;85(2):204-209.
- McNab AA, Wright JE. Orbitofrontal cholesterol granuloma. Ophthalmology. 1990; 97: 28-32.
- Denig R. Subperiosteal blood cyst of the orbit; report of a case. Ophthalmic Record 1902;11:187. Retrieved from https://books.google.com.ph/books?id=pSSgAAAAMA AJ&pg=PA179&dq=The+Ophthalmic+Record,+Vol.+1 1+1902&hl=en&newbks=1&newbks_redir=0&sa=X&ve d=2ahUKEwiFxYr23r2AAxV5d2wGHbFhCesQuwV6BAgHEAY#v=onepage&q=The%20Ophthalmic%20Reco rd%2C%20Vol.%2011%201902&f=false (accessed Aug 1, 2023).
- Santiago MDD, Sua AS. Cholesterol granuloma of the orbit. Philipp J Ophthalmol. 2005; 30(3):129–132.
- Hughes JD, Jacob JT, Garrity JA, Salomao DR, Link MJ. Orbitofrontal Cholesterol Granuloma: Four Case Reports and a Systematic Review of the English Literature. World Neurosurg. 2016 Mar;87:355-61.
- Parke DW 2nd, Font RL, Boniuk M, McCrary JA 3rd. ‘Cholesteatoma’ of the orbit. Arch Ophthalmol. 1982 Apr;100(4):612-6.